
Our Country’s Veteran Suicide Crisis
Our nation’s suicide epidemic takes a devastating toll on veterans.
Since 2006, veterans have died by suicide nearly 20 times more often than soldiers have been killed in war operations.1 These suicides overwhelmingly involve firearms.
The people who so bravely sacrificed to serve and protect our nation deserve better. Fortunately, these tragedies are preventable. By encouraging responsible firearm ownership practices and enacting strong gun safety laws, we can help our veterans—and all Americans—overcome this preventable public health crisis.
You are not alone. If you or a loved one are contemplating suicide, please call the free and confidential national Suicide & Crisis Lifeline by dialing 988 or access help through their website at 988lifeline.org.
Suicide is an urgent public health problem across the country. Each year, more than 48,000 people die from suicide—more than half of which involve firearms.2 American veterans disproportionately shoulder the burden of our nation’s gun suicide epidemic. More than 6,400 veterans die by suicide each year, and veterans account for roughly one in five firearm suicides in the US.3
For veterans and non-veterans alike, our country’s suicide problem is a gun problem. Over 71% of veteran suicides involve firearms, compared with roughly 53% of all suicides nationwide.4 The proportion of veteran suicides that are carried out with firearms has increased in recent years. In fact, in 2022, nearly 74% of veteran suicides involved firearms, the highest percentage on record.5
Background on Guns and Suicide
1 in 5 gun suicide victims are veterans
Source
“2019 National Veteran Suicide Prevention Annual Report,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, September 2019, https://www.mentalhealth. va.gov/docs/data-sheets/2019/2019_National_Veteran_Suicide_Prevention_Annual_ Report_508.pdf. See also, “National Suicide Data Report Appendix,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/ suicide_prevention/data.asp.
Firearms are the most lethal of the commonly available means of suicide in the US. The vast majority of people who attempt suicide survive—unless they use a gun. This lethality explains why less than five percent of non-firearm suicide attempts result in death, while approximately 85% of gun suicide attempts are fatal.6
Because of this unique lethality, easy access to firearms is one of the most salient risk factors for suicide. Research suggests that having a gun in the home triples a person’s overall risk of suicide.7 Nearly half of all veterans own firearms,8 compared to 30% of the general population.9
Importantly, however, gun suicide is preventable. Many suicide attempts are impulsive acts utilizing whatever methods are immediately available—48% of people harm themselves within 10 minutes of deciding to attempt suicide.10 Of those who survive a suicide attempt, the vast majority never attempt again, and 90% do not go on to die by suicide.11 By delaying and limiting access to guns among those at a proven risk of suicide, we can save thousands of American lives every year.
Trends in Veteran and Non-veteran Suicide
Over the last decade, the suicide rate for veterans has been much higher than the suicide rate of the general population. The veteran suicide rate is 2.6 times higher than the non-veteran adult suicide rate.12
Additionally, the veteran suicide rate has historically risen faster than the suicide rate for non-veterans. From 2008 to 2022, the veteran suicide rate increased by 32%, compared to a 20% increase for non-veterans.5
MEDIA REQUESTS
Our experts can speak to the full spectrum of gun violence prevention issues. Have a question? Email us at media@giffords.org.
Contact
Geography
Veteran suicide rates are highest in the Western states, followed by the Midwestern and Southern states.13 Veteran suicide rates are lowest in the in Northeastern states.14 However, firearms are used in the highest proportion of suicides in Southern states (62%), followed by Midwestern (56%), Western (51%), and Northeastern states (39%).14
In general, states which had the highest rates of veteran suicide saw a higher proportion of veteran suicides by firearm compared to states with lower rates of veteran suicide. For example, in 2022, Montana had the highest veteran suicide rate.14 Eighty-two percent of veteran suicides in the state that year involved firearms.14 Maryland had the lowest rate of veteran suicides that year. 14
Age
Although veterans of all ages die by suicide at higher rates than non-veterans of the same age, this disparity is most pronounced for 18–34 year old veterans, who died by suicide at nearly three times the rate of non-veterans the same age in 2022.14
Race and Ethnicity
Rates of suicide in 2021 were highest for American Indian/Alaska Native veterans, followed by white, Asian American, and Black veterans.15 Veterans of every racial group have higher suicide rates than the overall suicide rate by race: Asian American and Pacific Islander veterans die by suicide at nearly four times the overall Asian American and Pacific Islander suicide rate.14 Black, white, and American Indian/Alaska Native veterans die by suicide at twice the overall rate of their respective racial groups.16
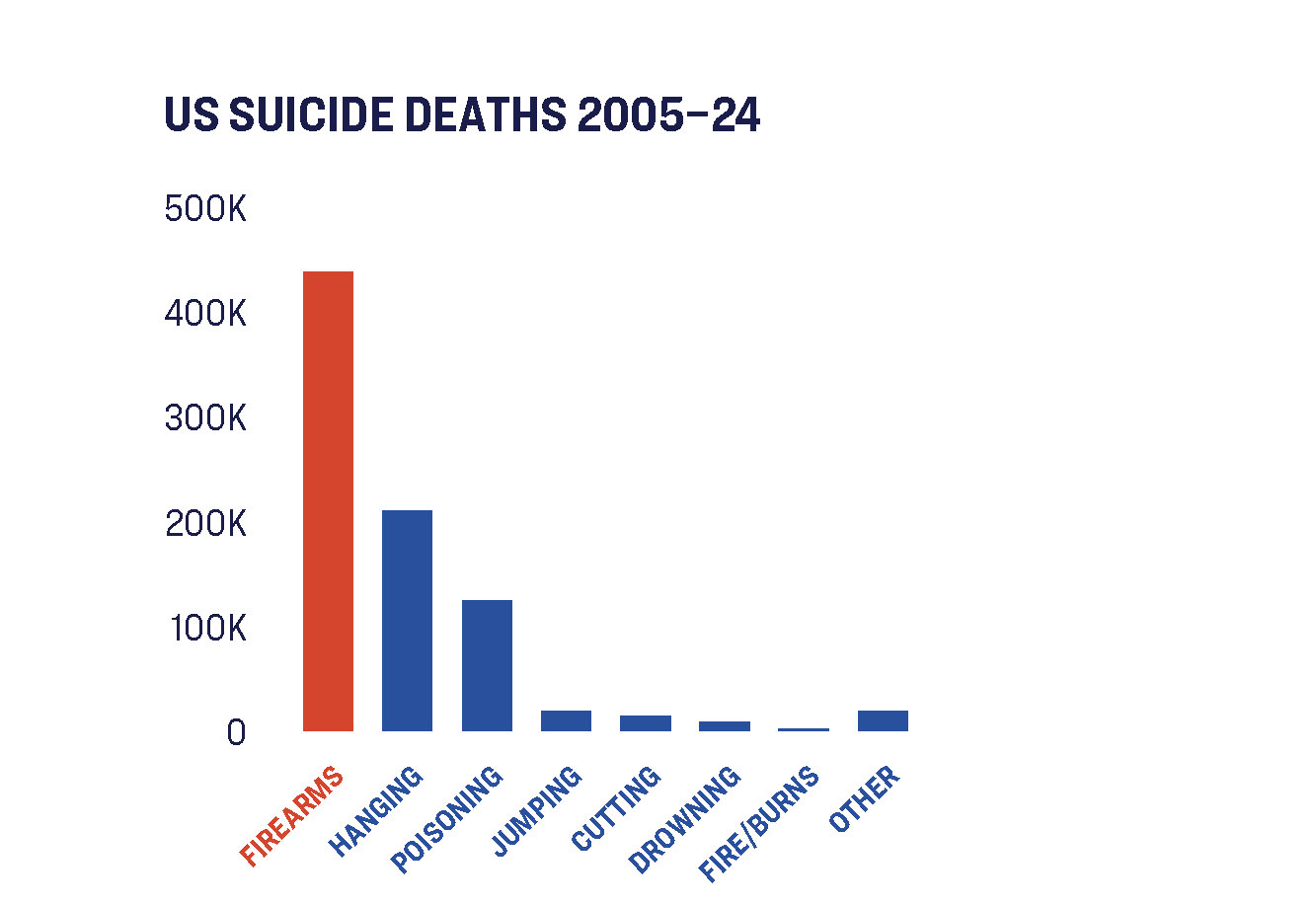
Guns are the most common method of suicide
Source
Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (WONDER), “Underlying Cause of Death, 2018-2024, Single Race,” last accessed February 25, 2026, https://wonder.cdc.gov/.
Veteran suicides also show substantial disparities for Hispanic and non-Hispanic veterans. Non-Hispanic veterans are 1.7 times as likely to die by suicide as Hispanic veterans.16
Sex
Both male and female veterans have higher suicide rates—and are more likely to use firearms in suicide attempts—than non-veterans of the same sex. In 2022, female veterans died by suicide at nearly twice the rate of non-veteran females; male veterans died by suicide at a rate 1.4 times higher than non-veteran males.17
One study found that male veterans were 41% more likely to use a firearm in suicide attempts relative to non-veteran males; female veterans were 39% more likely to use a firearm in suicide attempts relative to non-veteran females.18
LGBTQ Veterans
Understanding the Threat of Gun Violence for Transgender People
Mar 31, 2021
An estimated one million veterans in the United States are gay.19 Research suggests that these veterans face elevated risk of suicide compared to both their heterosexual veteran peers and the general population. In fact, in 2017, suicide was the fifth leading cause of death among gay, lesbian, and bisexual veterans, but the tenth leading cause of death in the general US population.20 Gay, lesbian, and bisexual veterans had a suicide rate more than twice as high as the general veteran population.14
Suicide also takes a disproportionate toll on transgender veterans. Transgender adults serve in the US military at two to three times the rate of the general adult population.21 However, transgender veterans die by suicide at twice the rate of their cisgender veteran peers22 and nearly six times the rate of the general population.23
To prevent veteran suicides, it is critical that we take steps to address the role that firearms play in this crisis. Veterans with firearms in their homes can work with friends, family members, clinicians, and others to develop a plan to reduce access to lethal means during times of crisis. There are a range of steps and related policies that can help address the risks associated with firearm access and prevent firearm suicide.
ENCOURAGE Physician Firearm Safety Counseling
Half of individuals, including veterans, who die by suicide are seen in primary care settings in the month prior to death.24 In fact, one survey of veterans already receiving mental health care found that nearly 56% of patients with a suicide plan had guns in the household.25 Clearly, medical professionals can play an important role in discussing suicide risk and firearms safety with patients.
A majority of Americans, including veterans, believe it is appropriate for physicians to have conversations about firearms in the clinical setting.26 However, despite this comfort and the disproportionate risk of suicide veterans face, a recent study found that fewer than one in 10 veteran firearm owners report ever having spoken with a clinician about firearm safety.27 These results suggest that additional efforts to facilitate such discussions are warranted.
Both veterans and clinicians emphasize that these conversations work best when they are personalized to the patient, emphasize the rationale for the conversation, and respect veterans’ unique relationship with firearms.28 Many resources have been developed to help clinicians feel more comfortable and capable of engaging in firearm safety conversations with veteran patients.29
IMPROVE Safe Firearm Storage
More than one-third of veterans who own guns store at least one of their firearms loaded and unlocked,30 lower than the 54% of all gun owners who store at least one gun unsafely.31 However, close to two-thirds of veteran gun owners store at least one gun unlocked, and 47% store at least one firearm loaded.30

Safe Storage Laws Save Lives
—Dec 09, 2021
Safe firearm storage—where guns are stored unloaded, locked up, and ammunition locked and stored separately—is an important way to disrupt access to lethal means in times of crisis. In fact, recent studies suggest that veterans in suicidal crisis are more likely than other veterans to store firearms unsafely. For example, one study found that veterans who used a firearm for suicide were more likely to have a documented unsecured firearm in their home at the time of their death.32 Another study of female veterans who served after 9/11 found that such veterans with lifetime or past month suicide ideation were more likely to store guns loaded.33
Promoting safety around lethal means and firearms is an important part of the Department of Veterans Affairs suicide prevention campaign. In the fall of 2021, the VA released a series of ads targeted at veterans that indicate that “a simple lock puts space between a thought and a trigger.”34
PROMOTE Temporary Out-of-Home Gun Storage
People at risk of suicide can often be active partners in promoting their own health and safety by taking voluntary steps to limit their own access to the most lethal means of suicide. In some cases, family, friends, therapists, or physicians can successfully convince a struggling person to temporarily and voluntarily store guns outside the home to make them less accessible in a moment of crisis.
Previous studies have found that many firearm retailers and law enforcement agencies are willing to offer or have offered temporary, voluntary firearm storage of firearms to prevent suicide and other firearm-related harms.35 Community activists and researchers in several states, including Colorado,36 Maryland,37 Mississippi,38 and Washington,39 have created firearm storage maps to help community members find options for voluntary out-of-home storage. Veterans and their families can use these resources to develop safety plans to help prevent firearm suicide.
ENACT Extreme Risk Laws

We Must Address Veteran Suicide. ERPOs Can Help Us Do That.
Apr 29, 2021
Extreme risk laws allow families, household members, or law enforcement officers to petition a court for an extreme risk protection order (ERPO) which temporarily restricts a person’s access to guns if they are deemed a danger to themselves or others. Nearly 80% of those contemplating suicide show concrete signs before a suicide attempt.40 Extreme risk laws empower those most likely to notice warning signs to help remove firearms from people at a high risk of suicide.
These laws have enormous lifesaving potential. Researchers estimate that for every 10 to 20 gun removals carried out under Connecticut and Indiana’s extreme risk law, one life was saved through an averted suicide.41 Additionally, in 44% of Connecticut’s firearm removal cases, the request for an order to remove a gun resulted in the subject receiving mental health treatment they might not otherwise have received.42
So far, 21 states—California, Colorado, Connecticut, Delaware, Florida, Hawaii, Illinois, Indiana, Maryland, Massachusetts, Michigan, Minnesota, Nevada, New Jersey, New Mexico, New York, Oregon, Rhode Island, Vermont, Virginia, and Washington—and Washington DC have passed extreme risk laws.
ENSURE STRONG BACKGROUND CHECK SYSTEMS
To prevent veteran suicides, it is also critical that we push back against proposals that will increase veteran suicide by weakening systems put in place to protect them.
Since 1998, because of the Brady Handgun Violence Prevention Act, the Department of Veterans Affairs (VA) has shared records on beneficiaries with appointed fiduciaries for inclusion in the National Instant Criminal Background Check System (NICS). The fiduciary appointment is based on a VA determination that the beneficiary is “mentally incompetent” under VA regulations. Common reasons for being deemed incompetent include exhibiting signs of PTSD, dementia, schizophrenia, or other mental health challenges and having suffered severe brain trauma that makes it impossible to manage personal affairs.
This appointment of a fiduciary prohibits veterans who have been found to lack the mental capacity to manage their own affairs from possessing a gun unless they can show that their ownership of a gun would not pose a public safety threat. The VA’s incompetency determination procedure includes strong due process considerations and provides the veteran multiple avenues through which this determination could be challenged and the veteran’s access to guns restored. These considerations include notice of the proposed determination and evidence supporting it, an opportunity to request a hearing, an opportunity to present evidence, including evidence from a medical professional or other person, of the beneficiary’s ability to manage their benefits, and the opportunity to be represented, including by counsel, at a hearing and to bring a medical professional or other person to provide testimony at the hearing.
The NICS background checks system is one of the most effective and important tools we have to prevent people from accessing firearms who shouldn’t have them. The policies below would undermine the lifesaving work of the background checks system and the Veterans Administration.
- Failing to Report Veterans Who Present a Risk to NICS: Proposals that would prohibit the VA from reporting to NICS beneficiaries deemed “mentally incompetent” by the VA on the basis of being assigned a fiduciary to manage their affairs due to injury or disease place veterans at even further risk.
- Removing Veterans at Risk from NICS: Proposals to retroactively remove hundreds of thousands of VA records from NICS are even more dangerous. These proposals would allow beneficiaries previously deemed “mentally incompetent” by the VA on the basis of being assigned a fiduciary to manage their benefits to purchase and possess firearms. They would remove a key safety measure and allow access to firearms for a person even if they are in a state of crisis.
Far too many of our nation’s veterans have died at their own hands, and firearms have overwhelmingly been the means by which they have done so. Our nation’s veterans have bravely volunteered to risk their lives to fight for our country, and we owe them and their families meaningful action to address this crisis.
Now is the time for our leaders to show courage and pass the gun safety reforms that address the role that firearms play in fueling our nation’s suicide crisis.
JOIN OUR COALITION
If you’re a veteran who wants to lend their voice to this fight, we want to hear from you. Sign up to join our movement.

- Calculated by Giffords Law Center comparing the number of Overseas Contingency Operations (OCO) deaths and veteran suicide deaths. From 2006 to 2021, 4,620 service-members were killed in OCO operations. From 2006 to 2020, 127,560 veterans died by suicide. Giffords Law Center included an estimate of 6,000 veteran suicides for 2021, to create comparable years of data. Hannah Fischer and Hibbah Kaileh, “Trends in Active-Duty Military Deaths From 2006 Through 2021,” Congressional Research Service, September 9, 2022, https://sgp.fas.org/crs/natsec/IF10899.pdf; “National Suicide Data Report Appendix, 2022” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩]
- Based on an average of the five most recent years of available data: 2019-2023. Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (WONDER), “Fatal Injury Data,” last accessed April 30, 2024, https://wonder.cdc.gov/Deaths-by-Underlying-Cause.html.[↩]
- Based on an average of the five most recent years of available data: 2018-2022. “National Suicide Data Report Appendix, 2024” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩]
- “National Suicide Data Report Appendix, 2024” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp; Centers for Disease Control and Prevention, Wide-ranging Online Data for Epidemiologic Research (WONDER), “Fatal Injury Data,” last accessed April 30, 2024, https://wonder.cdc.gov/Deaths-by-Underlying-Cause.html.[↩]
- “National Suicide Data Report Appendix, 2024” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩][↩][↩]
- Matthew Miller, Deborah Azrael, and Catherine Barber, “Suicide Mortality in the United States: the Importance of Attending to Method in Understanding Population-Level Disparities in the Burden of Suicide,” Annual Review of Public Health 33 (2012): 393–408.[↩]
- Andrew Anglemyer, Tara Horvath, and George Rutherford, “The Accessibility of Firearms and Risk for Suicide and Homicide Victimization Among Household Members: a Systematic Review and Meta-analysis,” Annals of Internal Medicine 160, no. 2 (2014): 101–110.[↩]
- Emily C. Cleveland et al., “Firearm Ownership among American Veterans: Findings from the 2015 National Firearm Survey,” Injury Epidemiology 4, no. 1 (2017).[↩]
- Katherine Schaeffer, “Key Facts About Americans and Guns,” Pew Research Center, September 13, 2021, https://www.pewresearch.org/fact-tank/2021/09/13/key-facts-about-americans-and-guns/.[↩]
- Eberhard A. Deisenhammer et al., “The Duration of the Suicidal Process: How Much Time Is Left for Intervention Between Consideration and Accomplishment of a Suicide Attempt?,” The Journal of Clinical Psychiatry 70, no. 1 (2008): 19–24.[↩]
- David Owens, Judith Horrocks, and Allan House, “Fatal and Non-fatal Repetition of Self-Harm: Systematic Review,” The British Journal of Psychiatry 181, no. 3 (2002): 193–199.[↩]
- Based on 2022 data. “2024 National Veteran Suicide Prevention Annual Report,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, September 2024, https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf.[↩]
- “2024 State-Level Veteran Suicide Data: State Data Appendix,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩]
- Id.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- 2022 State-Level Veteran Suicide Data: State Data Appendix,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩]
- Based on 2020 data. Id.[↩][↩]
- “2024 National Suicide Data Report Appendix,” US Department of Veterans Affairs, Office of Mental Health and Suicide Prevention, https://www.mentalhealth.va.gov/suicide_prevention/data.asp.[↩]
- Adam G. Horwitz et al., “Characteristics of Veteran and Civilian Suicide Decedents: A Sex–Stratified Analysis,” American Journal of Preventive Medicine 56, no. 5 (2019): e163–e168.[↩]
- “Veterans with Lesbian, Gay, Bisexual and Queer Identities,” Community Provide Toolkit, US Department of Veterans Affairs, last accessed October 31, 2022, https://www.mentalhealth.va.gov/communityproviders/veterans-lgb.asp.[↩]
- Kristine E. Lynch, “Evaluation of Suicide Mortality Among Sexual Minority US Veterans from 2000 to 2017,” JAMA Network Open 3, no. 12 (2020): e2031357–e2031357.[↩]
- Jack Harrison-Quintana and Jody L. Herman, “Still Serving in Silence: Transgender Service Members and Veterans in the National Transgender Discrimination Survey,” LGBTQ Policy Journal 3, no. 1 (2013): 1–13.[↩]
- Taylor L. Boyer et al., “Suicide, Homicide, and All–cause Mortality Among Transgender and Cisgender Patients in the Veterans Health Administration,” LGBT Health 8, no. 3 (2021): 173–180.[↩]
- Raymond P. Tucker, “Suicide in Transgender Veterans: Prevalence, Prevention, and Implications of Current Policy,” Perspectives on Psychological Science 14, no. 3 (2019): 452–468.[↩]
- Lauren M. Denneson et al., “Suicide Risk Documented During Veterans’ Last Veterans Affairs Health Care Contacts Prior to Suicide,” Suicide and Life-Threatening Behavior 46, no. 3 (2016): 363–374; Jason B. Luoma, Catherine E. Martin, and Jane L. Pearson, “Contact with Mental Health and Primary Care Providers Before Suicide: a Review of the Evidence,” American Journal of Psychiatry 159, no. 6 (2002): 909–916.[↩]
- Marcia Valenstein et al., “Possession of Household firearms and Firearm–related Discussions with Clinicians Among Veterans Receiving VA Mental Health Care,” Archives of Suicide Research (2019).[↩]
- Marian E. Betz, Deborah Azrael, Catherine Barber, and Matthew Miller, “Public Opinion Regarding Whether Speaking with Patients About Firearms is Appropriate: Results of a National Survey,” Annals of Internal Medicine 165, no. 8 (2016): 543–550; Summer Newell et al., “Veterans are Agreeable to Discussions About Firearms Safety in Primary Care,” The Journal of the American Board of Family Medicine 34, no. 2 (2021): 338–345.[↩]
- Joseph A. Simonetti et al., “Receipt of Clinician-delivered Firearm Safety Counseling Among US Veterans: Results from a 2019 National Survey,” Suicide and Life-Threatening Behavior (2022).[↩]
- Summer Newell et al., “Veterans are Agreeable to Discussions About Firearms Safety in Primary Care,” The Journal of the American Board of Family Medicine 34, no. 2 (2021): 338–345; Steven K. Dobscha et al., “Strategies for Discussing Firearms Storage Safety in Primary Care: Veteran Perspectives,” Journal of General Internal Medicine 36, no. 6 (2021): 1492–1502.[↩]
- See, e.g., Jennifer L. Bryan et al., “A High–need, High-impact Educational Session on Firearms and Death by Suicide,” Suicide and Life-Threatening Behavior (2021).[↩]
- Joseph A. Simonetti, Deborah Azrael, Ali Rowhani-Rahbar, and Matthew Miller, “Firearm Storage Practices Among American Veterans,” American Journal of Preventive Medicine 55, no. 4 (2018): 445–454.[↩][↩]
- Cassandra K. Crifasi et al., “Storage Practices of US Gun Owners in 2016,” American Journal of Public Health 108, no. 4 (2018): 532–537.[↩]
- Brooke A. Ammerman and Mark A. Reger, “Evaluation of Prevention Efforts and Risk Factors Among Veteran Suicide Decedents who Died by Firearm,” Suicide and Life-Threatening Behavior 50, no. 3 (2020): 679–687.[↩]
- Lindsey L. Monteith et al., “Prevalence and Correlates of Firearm Access Among Post-9/11 US Women Veterans Using Reproductive Healthcare: a Cross-sectional Survey,” Journal of General Internal Medicine 37, no. 3 (2022): 714–723.[↩]
- Leo Shane III, “VA Zeroes in on Gun Safety as a Way to Reduce Veteran Suicides,” Military Times, September 22, 2021, https://www.militarytimes.com/veterans/2021/09/22/va-zeroes-in-on-gun-safety-as-a-way-to-reduce-veteran-suicides/.[↩]
- Carol W. Runyan et al., “Law Enforcement and Gun Retailers as Partners for Safely Storing Guns to Prevent Suicide: A Study in 8 Mountain West States,” American Journal of Public Health 107, no. 11 (2017): 1789–1794.[↩]
- Colorado Firearm Safety Coalition, “Gun Storage Map,” https://coloradofirearmsafetycoalition.org/gun-storage-map/.[↩]
- Marylanders to Prevent Gun Violence, “Maryland Safe Storage Map,” https://mdpgv.org/safestoragemap/.[↩]
- University of Southern Mississippi, “Mississippi Gun Storage Map,” http://mikeanestis.weebly.com/ms-gun-storage-map.html.[↩]
- Harborview Injury Prevention and Research Center, “Washington Firearm Safe Storage Map,” https://hiprc.org/firearm/firearm-storage-wa/.[↩]
- Robert N. Golden and Fred Peterson, The Truth about Illness and Disease (Infobase Publishing, 2009), 53.[↩]
- Jeffrey W. Swanson et al., “Implementation and Effectiveness of Connecticut’s Risk–based Gun Removal Law: Does it Prevent Suicides,” Law & Contemporary Problems 80, (2017): 179–208; Jeffrey W. Swanson et al., “Criminal Justice and Suicide Outcomes with Indiana’s Risk-Based Gun Seizure Law,” The Journal of the American Academy of Psychiatry and the Law, (2019).[↩]
- Jeffrey W. Swanson et al., “Implementation and Effectiveness of Connecticut’s Risk–based Gun Removal Law: Does it Prevent Suicides,” Law & Contemporary Problems 80, (2017): 179–208.[↩]